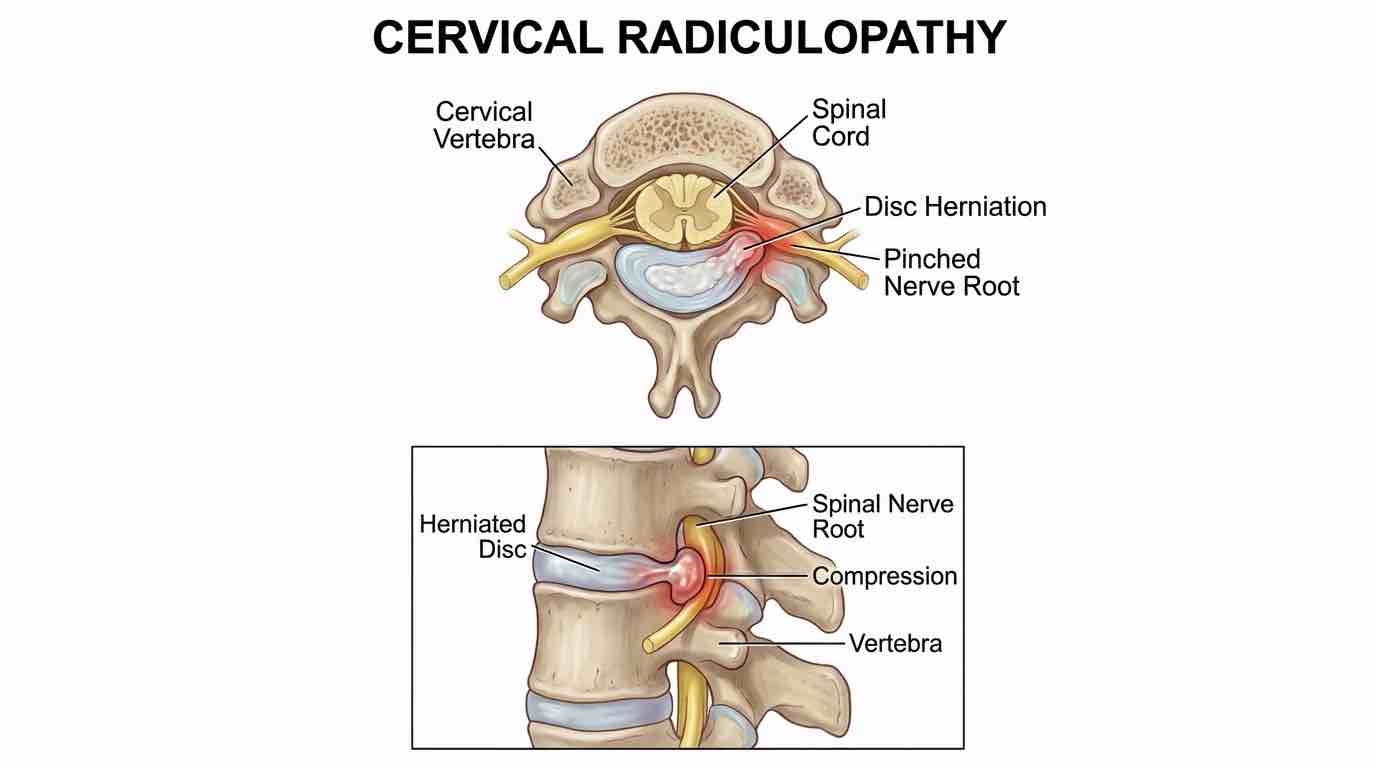
What is cervical Radiculopathy (pinched nerve in the neck)?
Cervical Radiculopathy is neurological dysfunction caused by pressure on a cervical nerve root in the neck. This pressure (or inflammation) interferes with the nerve’s ability to send signals, resulting in symptoms along the nerve’s pathway. The Mayo Clinic explains that Radiculopathy refers to symptoms from any spinal nerve compression – most often due to a herniated disk or degenerative spine changes. In the neck, this means any structural issue (like a bulging disc or osteophyte) pinching a nerve can produce arm or shoulder symptoms.
What is the cervical spine?
The cervical spine is the upper portion of the backbone that forms your neck. It consists of seven small vertebrae (labeled C1 through C7) stacked between your skull and upper back. These bones support the head, protect the spinal cord, and allow you to turn your neck. Between each vertebra lies a shock-absorbing disc. The spinal cord and nerve roots pass through this column of bones. Each cervical nerve root branches out and extends into specific areas: shoulders, arms, chest, and upper back. In other words, a problem at a given vertebra or disc level affects the parts of the body served by that nerve. For example, a pinched C6 nerve might cause symptoms in the shoulder and thumb. When a cervical nerve root is compressed or irritated, pain or tingling can “radiate” along that nerve’s pathway from the neck into the arm.
Symptoms
Patients with cervical Radiculopathy typically experience neck and arm pain accompanied by nerve symptoms. Common symptoms include:
Radiating Pain: Sharp, burning or “electric” pain that starts in the neck and shoots down the shoulder or arm. It often follows the specific nerve’s distribution (e.g. into the thumb or hand).
Numbness & Tingling: A “pins-and-needles” sensation or loss of feeling in the shoulder, arm, or hand. For example, the inner forearm or fingers may tingle or go numb.
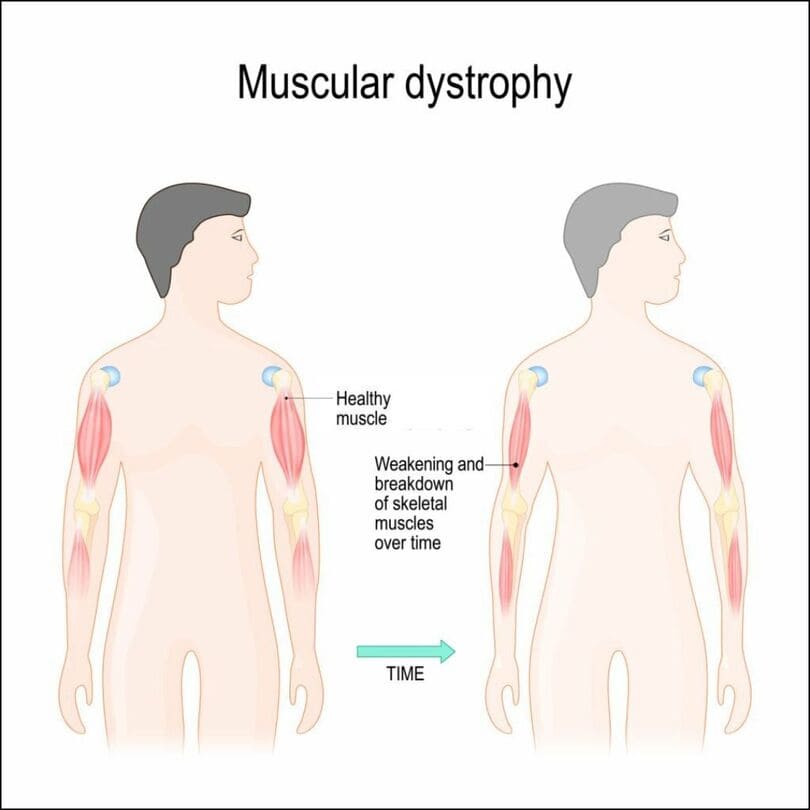
Muscle Weakness: The affected arm or hand muscles may feel weak or clumsy. Patients often notice decreased grip strength or difficulty lifting objects.
Reduced Reflexes: Tendon reflexes (e.g. the biceps or triceps reflex) can be diminished on the affected side.
Most cases affect only one side of the body – for example, your right arm but not your left. Neck movement (like looking up or down) may worsen pain, while supporting the arm (even resting a hand on the head) can sometimes ease the symptoms. In short, cervical radiculopathy often feels like a combination of neck pain plus arm pain/numbness, localized to the distribution of the compressed nerve.
Causes and Risk Factors
Cervical radiculopathy results from pressure on a neck nerve root. The two most common causes are:
Age-related degeneration (cervical spondylosis): Over time, spinal discs dehydrate and shrink, and bone spurs (osteophytes) can form. This “wear-and-tear” arthritis of the neck narrows the foramen (nerve exit holes) and pinches the nerve. In fact, Cleveland Clinic notes that degenerative changes are the most common cause in older adults.
Herniated (bulging) cervical disk: In younger to middle-aged people, a sudden strain or repetitive stress can cause a disc to bulge or rupture. The inner gel (nucleus) of the disc can then press on nearby nerve roots. For instance, bending the neck forward or lifting a heavy object may force the disc material into the spinal canal.
Other, less common causes include tumors or infections (which enlarge structures in the canal), and traumatic injuries. Risk factors increase the likelihood of these causes and include: heavy manual labor or jobs with constant neck strain, occupations involving vibrating machinery or driving, poor posture (e.g. prolonged “forward head” at a desk), and smoking (which accelerates disc degeneration). Sports injuries or motor vehicle accidents (whiplash) are common triggers as well. In short, any activity that forces the neck into awkward positions or accelerates spinal wear can set the stage for a pinched neck nerve.
Herniated Disks and Cervical Radiculopathy
A herniated cervical disk is a frequent culprit in younger patients. Normally, spinal discs cushion between vertebrae. If a disc’s tough outer ring (annulus) tears, the softer center (nucleus pulposus) can slip out. When this leaking disc material protrudes into the spinal canal, it can press directly on a nerve root, causing Radiculopathy. Mayo Clinic confirms that most radiculopathy cases involve disk herniation or spine degeneration. Factors like age, repetitive neck movements, poor posture, or trauma contribute to herniation. For example, bending the neck forward compresses the front of the vertebrae, which can force a disc backward toward the nerves. If the disc cracks open on the side adjacent to a nerve exit, the gel-like material pushes against the nerve root. The result is painful pressure on that nerve.
Cervical Radiculopathy from a herniated disk often affects adults under 50, and symptoms may come on abruptly if the tear is acute. As Cleveland Clinic notes, chemicals from the torn disc and the mechanical pressure both irritate the nerve, causing pain, numbness or tingling along the arm. The exact symptoms depend on which nerve root is pinched (for example, a C5 nerve herniation can cause shoulder and upper arm pain, while a C8 nerve issue can affect the hand and fingers).
Management and Treatment
Most people with cervical radiculopathy improve with nonsurgical treatment. According to Cleveland Clinic, over 85% of cases get better in 8–12 weeks with conservative care. Initial management aims to relieve nerve irritation and control pain:
Immobilization and Rest: A short period of rest and use of a soft cervical collar can limit painful motion. (Collars are typically only used for a week or two to avoid weakening neck muscles.)
Medications: Nonsteroidal anti-inflammatories (NSAIDs like ibuprofen) or a brief course of oral corticosteroids help reduce inflammation around the nerve. These are taken under a doctor’s guidance. Muscle relaxants or neuropathic pain medications (like gabapentin) may also be used if needed.
Physical Therapy and Exercises: This is a cornerstone of recovery. A physiotherapist or osteopath guides the patient through targeted neck exercises to improve posture, strengthen supporting muscles, and increase flexibility. Manual therapies (gentle massage, mobilization) can reduce muscle tension around the nerve. Proper ergonomics and posture correction are taught to prevent future strain. (For many patients, pain decreases as they progress through range-of-motion exercises into more advanced strengthening.)
York Rehab Clinic (Richmond Hill) Treatments: At York Rehab Clinic, our Richmond Hill team offers comprehensive rehabilitation for cervical Radiculopathy. We provide hands-on physiotherapy and osteopathy to mobilize the spine and correct posture, along with gentle chiropractic adjustments for alignment. Our registered massage therapists (RMT) use soft-tissue work to relax tight neck and shoulder muscles. We also offer advanced modalities: laser therapy and shockwave therapy to promote healing, and specialized cervical decompression (spinal decompression) to gently relieve disc pressure. Patients can also receive acupuncture or PRP pain management for additional relief. All these services are available on-site in Richmond Hill; York Rehab Clinic’s team tailors a treatment plan to your specific nerve injury.
Lifestyle Modification: We educate patients on avoiding aggravating positions and maintaining healthy habits – for example, taking breaks from desk work to move the neck, doing stretching routines, and using proper lifting techniques. Maintaining a healthy weight and quitting smoking also support spine health.
If symptoms persist beyond 6–12 weeks or worsen despite therapy, more intensive interventions may be considered. These include cervical epidural steroid injections (which bathe the nerve in anti-inflammatory medication) and, as a last resort, surgical options to remove pressure on the nerve. Your healthcare provider will discuss these options if needed.
at relieving nerve pressure and restoring function.
Advanced Care: If conservative care fails, injections or surgery may be needed